2005 Testimony
Testimony Before the Senate Appropriations
Senator Holmberg, Chairman
HB 1012 - DHS Budget - Medical Services Budget Area
March 1, 2005
Chairman Holmberg, members of the committee. I am David Zentner, Director of Medical Services for the Department of Human Services. I appear before you to provide an overview of the programs administered by my Division with the exception of long-term care.
Programs
The Medical Services Division administers three programs, they are Medicaid, the State Children's Health Insurance Program (Healthy Steps), and Children's Special Health Services (CSHS). This area of the budget provides public health care coverage for families and children, pregnant women, the elderly, and disabled citizens of our state.
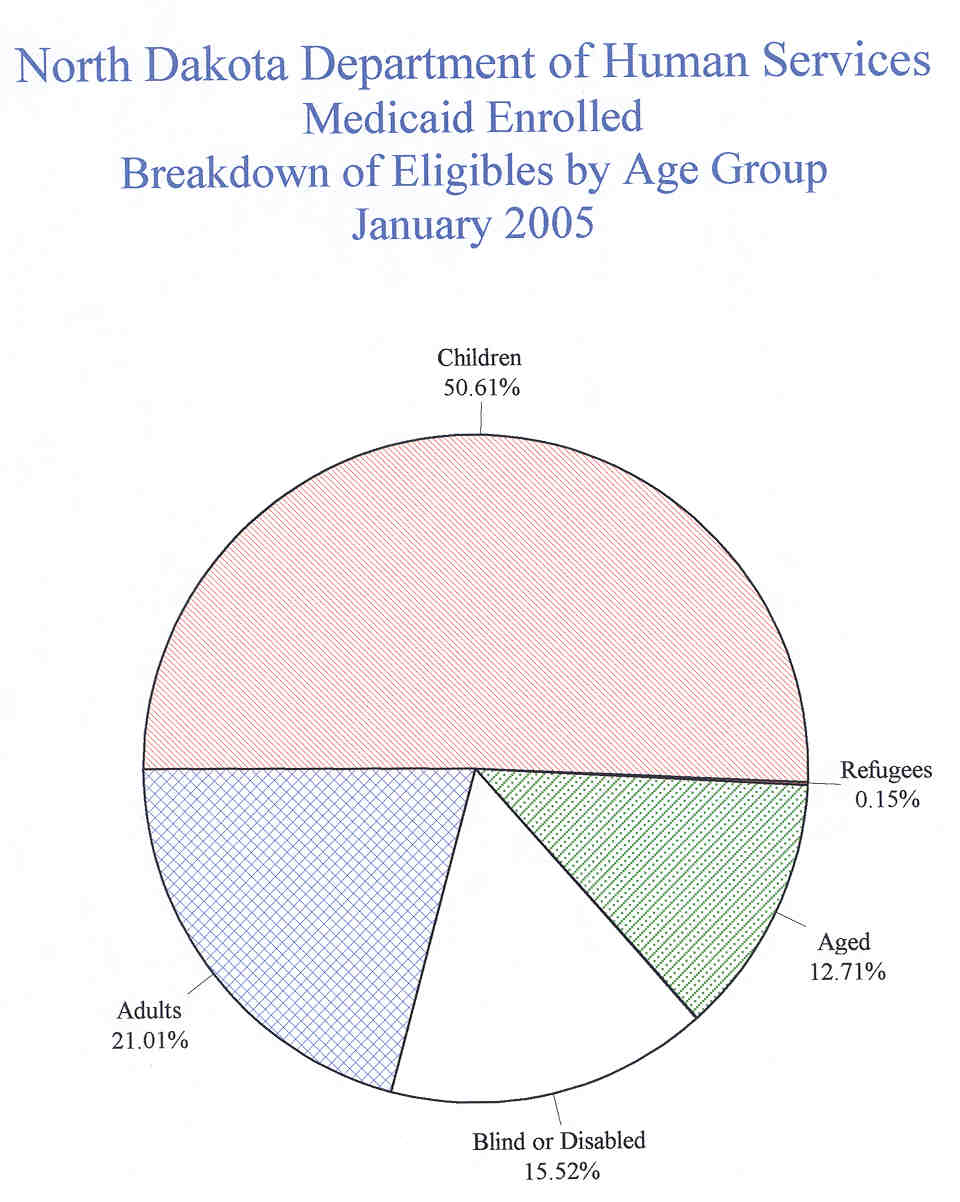
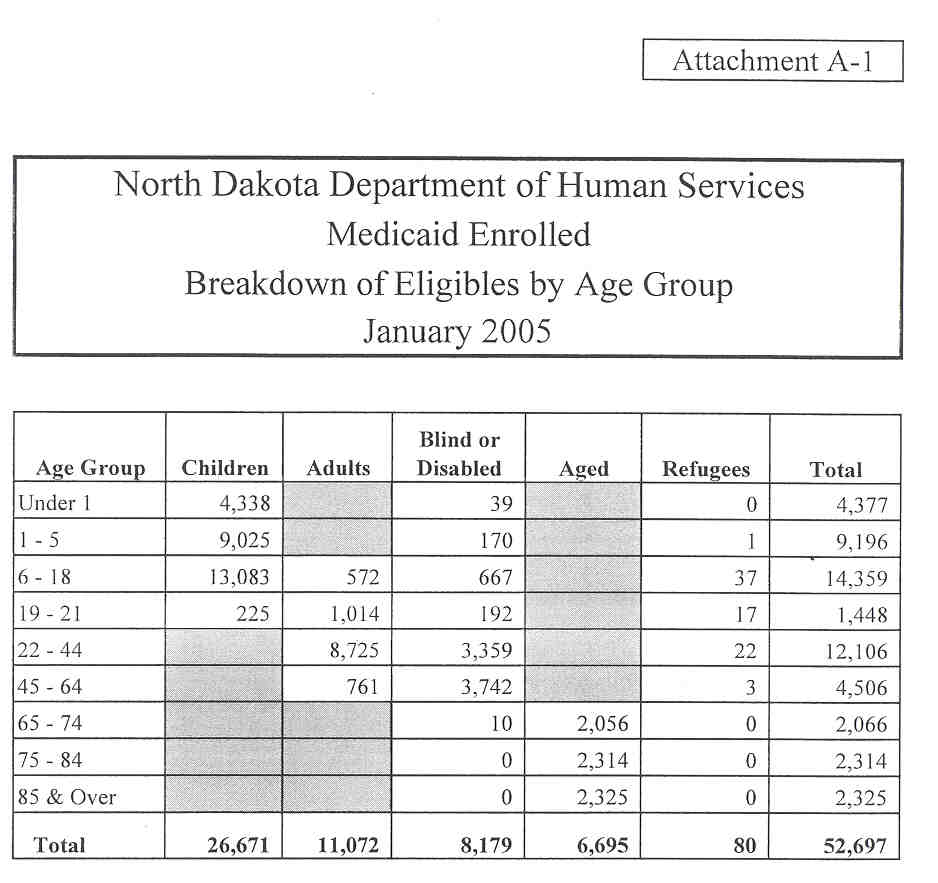
Medicaid is by far the largest portion of the budget. As of November 30, 2004, a total of 52,300 individuals were enrolled in the program. Attachment A shows the number of enrolled Medicaid recipients in November by category, and Attachment B shows the number of enrolled recipients and the number of recipients for whom a payment was made since the start of the current biennium. Attachment C details the number of children enrolled in Healthy Steps since the beginning of the current biennium. In addition, about 300 children had health care services paid on their behalf through CSHS during the year ending June 30, 2004. An additional 1,039 children received assistance through specialty clinics and information and referral services.
Program Trends
The overall economy in North Dakota has seen a marked improvement over the last several years. The Federal Medical Assistance Percentage (FMAP) is calculated based on per capita income over a three-year period. As a result, the FMAP for North Dakota has dropped considerably over the past two years, and it is anticipated that it will continue to fall through at least 2007. The current FMAP is 67.49%. The percentage will drop to 65.85% for the 2006 federal fiscal year beginning on October 1, 2005. It is anticipated that it will further decline to about 63.23% for the 2007 federal fiscal year that begins on October 1, 2006. The impact to the Department's budget as a result of this FMAP reduction totals about $32 million of which about $11.0 million is directly related to services covered in my testimony today.
Health care becomes an ever-evolving process that produces new prescription drugs, new diagnostic tools, and new sophisticated treatments and surgical procedures. While these changes often result in dramatic breakthroughs in treatment, they are in many instances expensive and therefore increase the overall cost of delivering services throughout the health care system. This trend will likely continue into the foreseeable future.
While the number of individuals eligible for the programs administered by Medical Services has leveled off, we note that many have chronic conditions that require extensive treatment. We see this trend continuing, and we are interested in instituting disease management to improve the health outcomes of those individuals who have high medical costs, while at the same time trying to reduce overall costs to the program over time. House Bill 1459 requires the Department to implement such a plan for the most costly 2,000 recipients in the Medicaid Program. The House Appropriations Committee also included additional administrative funds to implement this initiative.
Medicaid is the single largest payer of mental health services in the nation. Many individuals with severe mental conditions rely on Medicaid for services. For example, of the top 20 highest cost drugs paid through the Medicaid Program, 13 are related to mental illness conditions. After Medicare Part D becomes reality in January 2006, the percentage of drugs paid for by Medicaid to treat mental illness will further increase because the elderly will no longer receive their drugs through the Medicaid program. We are the primary payer for individuals who are severely mentally ill. Across the nation about 50% of the costs related to these diagnoses are paid by Medicaid, and this trend is expected to continue into the foreseeable future. It behooves us to continue to improve the efficiency and effectiveness of delivery of services to this population.
We have seen a steady decline in our ability to serve our customers because of our current payment system. The current Medicaid Management Information System became operational in 1978. While it has served us well in the past it is imperative that we develop a new system during the next biennium. Without a new system we will continue to struggle to ensure prompt and accurate payment of claims, struggle to institute changes that will improve our ability to monitor the delivery of services, and struggle to evaluate information to ensure the overall integrity of the Medicaid program. You were presented a more detailed explanation of that need in my earlier testimony.
Performance Measures
While we have experienced some delays in processing claims, staff has still been able to process the vast majority of claims within 30 days of receipt in our office. Most pharmacy claims are processed within a week because of the point of sale process used to pay these claims. The charts below indicate our progress to meet our goal of processing 90% of our claims within 30 days, and 99% of our claims within 90 days of arrival in our office. We have made great strides in reducing the backlog, and as of November 2004, 94% of claims have been processed within 30 days.


CY 2004 through September 2004
In addition it is imperative that claims are processed in an accurate manner. The North Dakota Medicaid program participated in a pilot project with the federal government to determine the accuracy of claims processed during 2002 and 2003. The results of that pilot program, based on a scientific sample of claims, revealed that our accuracy rate was high.

Another major goal is to ensure that our children receive appropriate preventive and treatment services. Our Health Tracks screening program for children through age 21 is designed to detect problems early, and provide treatment before their conditions deteriorate and become more expensive to treat. The following chart details the results of our efforts to improve the number of children who are screened through this program.

Budget Changes
The following information provides detail and comparison of the current biennium appropriated funds with the amount requested for the new biennium, and the changes made by the House.
| 2003-2005 Budget | Increase / Decrease | 2005-2007 Request | House Changes | Request to Senate |
|
|---|---|---|---|---|---|
| Salaries | 5,216,578 | 583,194 | 5,799,772 | (126,676) | 5,673,096 |
| Operating | 4,685,177 | 136,054 | 4,821,231 | 70,947 | 4,892,178 |
| MA Grants | 372,882,755 | 21,102,433 | 393,985,188 | 1,240,292 | 395,225,480 |
| Total | 382,784,510 | 21,821,681 | 404,606,191 | 1,184,563 | 405,790,754 |
| General | 90,706,244 | 17,638,543 | 108,344,787 | 464,960 | 108,809,747 |
| Federal | 269,783,775 | 554,626 | 270,338,401 | 859,204 | 271,197,605 |
| Other | 22,294,491 | 3,628,512 | 25,923,003 | (139,601) | 25,783,402 |
| FTE | 59.0 | 2.0 | 61.0 | (1.0) | 60.0 |
The grant line item in the Executive Budget for the Medicaid and the Healthy Steps programs total $391.2 million, of which $103.9 are general funds, and $25.4 million are other funds. It includes $1.3 million, of which $.4 million is state funds to allow individuals to set aside an additional $2,500 for funeral expenses. Also included in the grants line item is $1.7 million, of which about $.4 million is retained funds for nursing facility surveys, and nurse aide registry, and $1.1 million, of which about $.4 million is state funds for Children's Special Health Services programs.
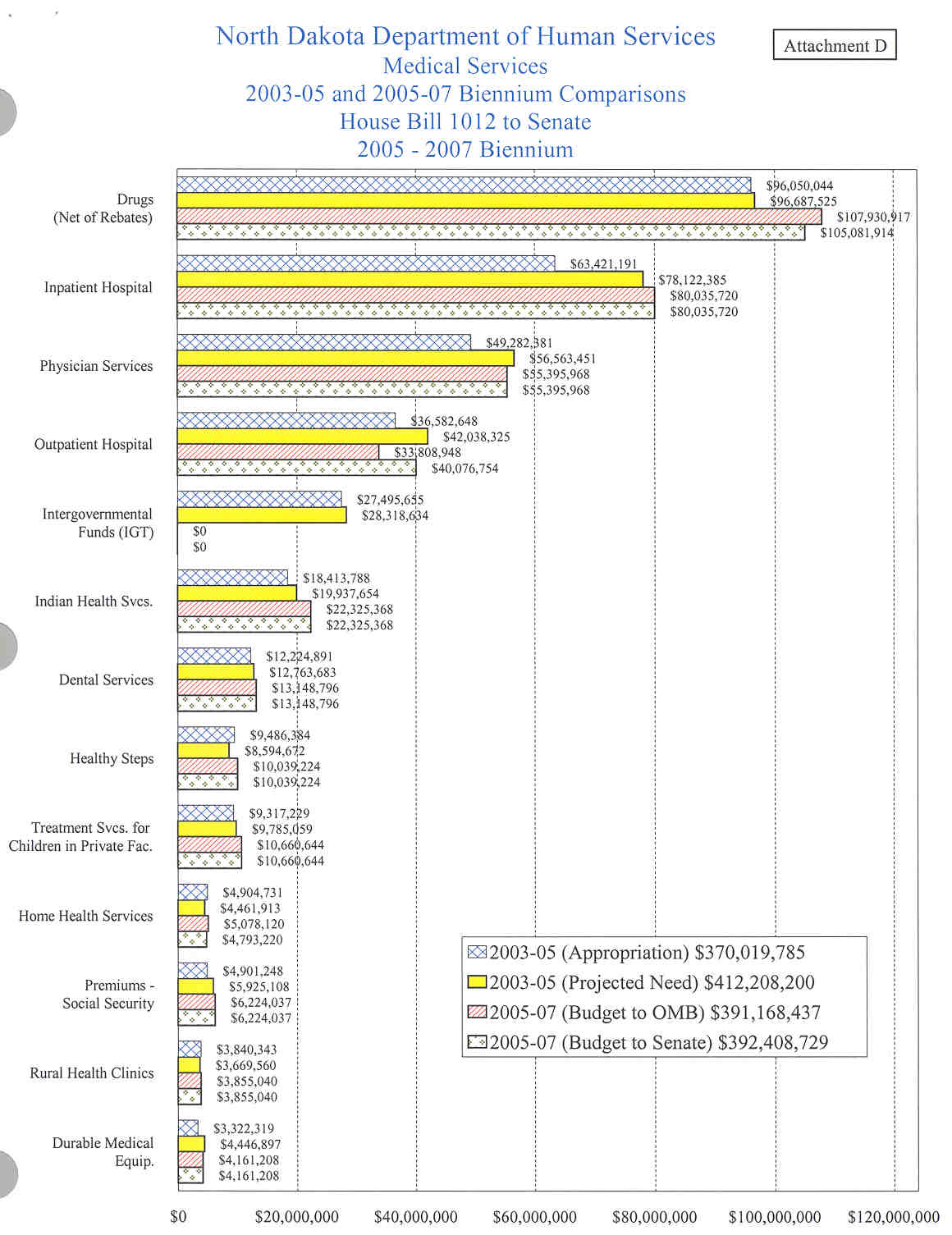
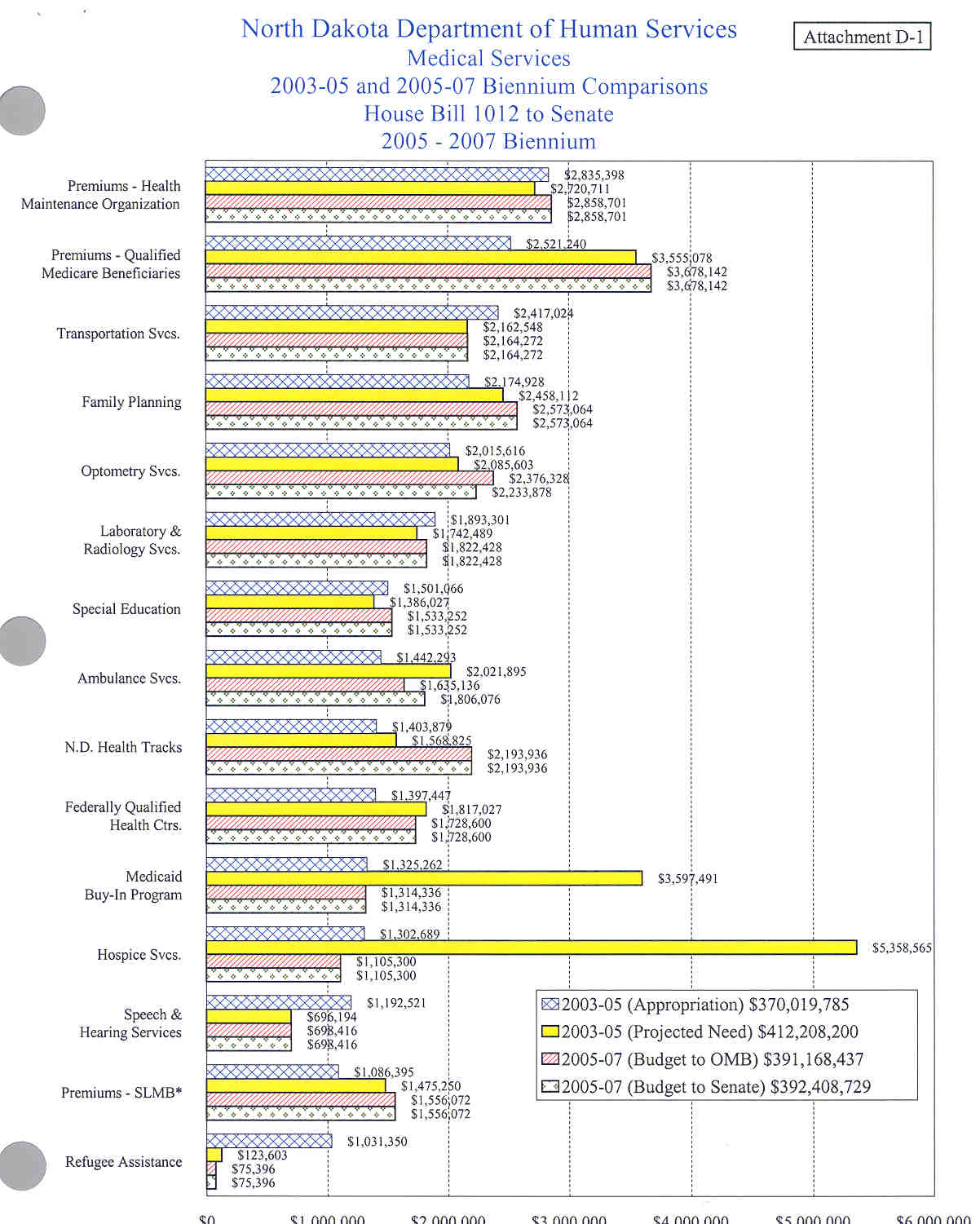
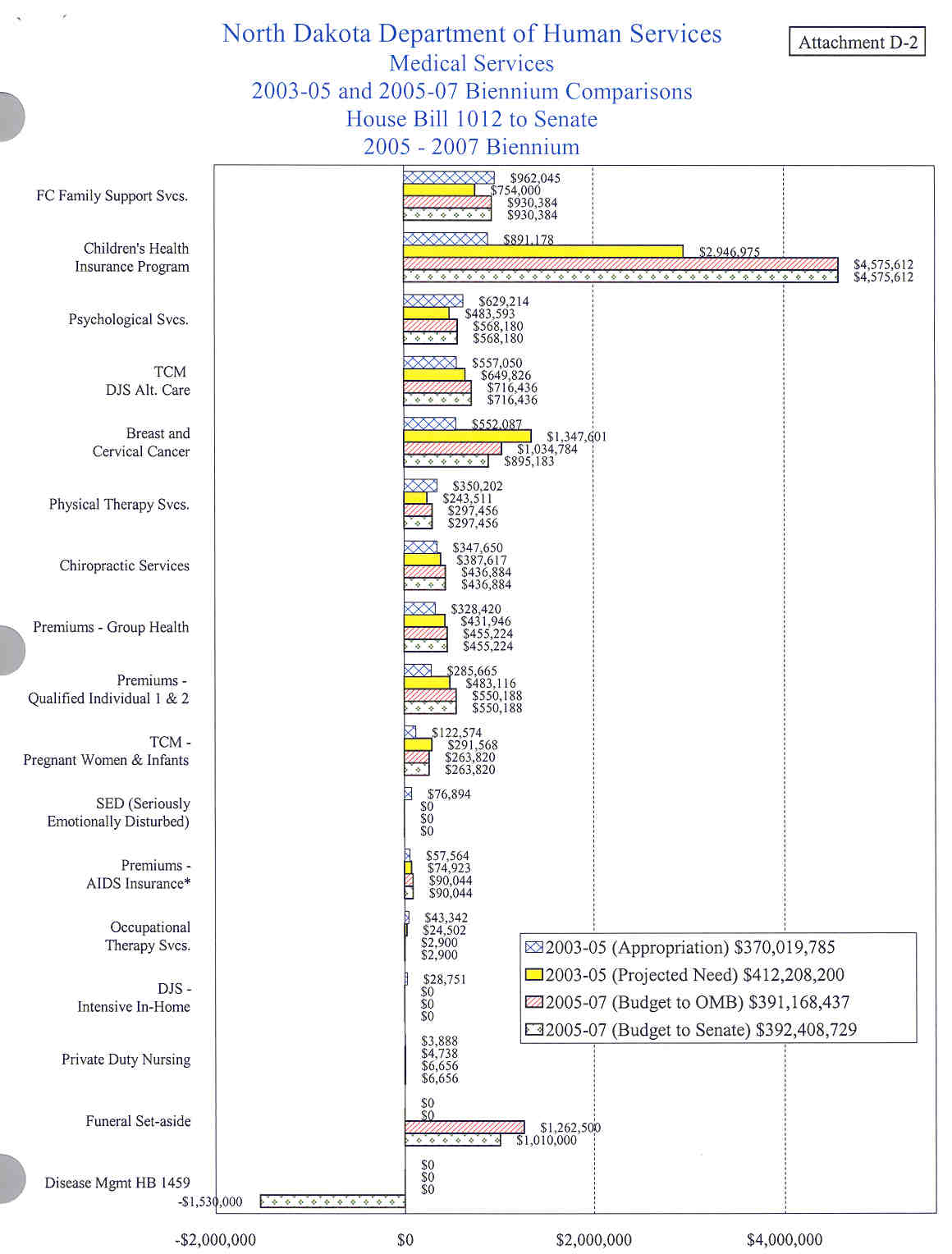
This budget does not include any Intergovernmental Transfer (IGT) funding because this program was phased out as of July 2004, in accordance with federal regulations. The current biennium appropriation for the Medicaid and Healthy Steps programs totals $370.0 million of which $27.5 million is IGT pool payments. For comparison purposes, if IGT pool payments are factored out of the current biennium the totals for the current biennium are $342.5 million of which $77.9 million are general funds and $21.6 million are other funds. When IGT pool payments are excluded, the requested increase totals $48.6 million in total funds and an increase of $26.1 million in general funds. Attachment D details the current appropriation, the anticipated expenditures for the current biennium, and the requested funding for the next biennium for each service.
Budget Highlights
- Due to the improving economy, the FMAP will be decreasing each federal fiscal year as noted in my comments above. This will result in the need for an additional $11.0 million just to maintain the program in its current form because of the drop in federal financial participation.
- This request includes provider inflationary increases of 2 percent per year for most services. The cost for this increase totals $6.9 million of which $2.4 million is state funds.
- Inpatient hospital services have trended much higher than anticipated at the beginning of the current biennium. This was caused primarily by an increase in the number of hospital admissions. We are requesting $80.0 million of which $28.1 million are state funds. This compares to $63.4 million of which $19.3 million are general funds in the current biennium.
- Physician services have also increased dramatically primarily due to an increase in the number of services provided by this group of providers. The actual units of service for the first year of the biennium were 27.2% greater than what was included in the current appropriation. We are requesting $55.4 million of which $19.4 million are state funds. This compares to $49.3 million of which $15.4 million are general funds in the current biennium.
- The prescription drug program is based on the assumption that the prior authorization program will continue to evolve, and that the other cost savings initiatives will remain in affect during the next two years. We are requesting, after drug rebates have been factored in, a total of $107.9 million of which $24.3 million are general funds and $14.1 million are retained funds. This compares to a current appropriation of $96.1 million, of which $16.2 million are general funds and $13.9 million are retained funds. Drug costs that are passed on to pharmacists by the drug manufacturers are generally higher than general medical inflation. In addition, new drugs that come onto the market often have high prices. You heard earlier that the budget was built on only one year of inflation which could result in a possible shortfall of funds for prescription drug services.
- We are requesting $10 million of which $2.5 million is state funds for the Healthy Steps program based on payment of 2,300 premiums per month. This amount includes a premium increase of 17.9% requested by Noridian Mutual Health Insurance Company. As of December 1, 2004, a total of 2,318 children were enrolled in the program.
- The Executive Budget request for administrative funding remains relatively unchanged. The operating expense request totaled $4.8 million, an increase of about $136,000 or a percentage increase of only 2.9%. The bulk of operating funds of $4.4 million or 92.5% will be used to pay for contracted services that include medical consultants, drug pricing, utilization, prior authorization, hospital utilization review, hospital audits, and inflation indicator information. The majority of increased costs are related to inflationary increases for these contracts.
- The salary and fringe benefit package includes 61 employees. These employees process 2.4 million claims per year, determine eligibility for the Healthy Steps Program, answer hundreds of calls per day from providers and other interested parties, develop and implement program policies for the three programs, conduct utilization review activities, establish payment and rate setting policies, provide screening services for children throughout North Dakota, oversee specialty clinics for children with special health care needs, distribute specialty food products for certain individuals with rare metabolic diseases, and many other tasks related to ensuring that we provide quality services to the clients, providers, and others that we serve.
- The original budget request included two new employees for the Medical Services Division. One position was for a pharmacist assistant that would help ensure that we collect the appropriate amount of drug rebates, assist in reviewing claims for accuracy and responding to written and verbal requests from providers, assist with the prior authorization process and help in monitoring the overall pharmacy program. The second position is an eligibility technician that will assist in the determining of eligibility for the Healthy Steps Program. At present one staff person determines eligibility for all Healthy Steps children. With the incorporation of Healthy Steps into the Vision system we anticipate additional workload to establish eligibility for this program. Eligibility for Healthy Steps is determined on a prospective basis and the additional staff person will ensure that new applications and renewals are processed before the end of each month in order to ensure that children do not lose health care coverage. In addition, the additional staff person will permit the Department to be better able to respond to requests for information from families and others who are interested in the program.
House Changes:
- The House deducted $18,138 of which $6,611 was from the general fund and $11,527 was from federal funds, from the salary line item. This changed the Governor's compensation package from providing a 4% increase on July 1, 2005, and a 3% increase on July 1, 2006, to a 3% increase on July 1, 2005, and a 4% increase on July 1, 2006.
- Salaries were further reduced by $20,000 of general funds as an allocated part of under-funding $600,000 of the department's pay plan.
- The operating line was decreased by $6,664 as an allocated part of a $50,000 general fund reduction to the Program and Policy section of the budget.
- The House reduced contract services by $475,550 of which $237,775 is general funds by removing the costs for a generic drug detailing process. The program that was started in conjunction with Nordian Mutual Health Insurance is designed to provide information and samples to physicians in an attempt to start Medicaid recipients on cost effective and therapeutically equivalent generic drugs rather than more expensive brand name drugs and counteract the physician detailing from drug manufacturer representatives that provide free samples of brand name drugs to physician offices. It was anticipated that this initiative could save a million dollars for every percentage switch from brand name to generic drugs. We request that you consider restoring these funds to the Medicaid budget.
- The House eliminated the pharmacy assistant position from the budget. We request that you consider adding back the position because we continue to believe the position is necessary to ensure that we continue to reduce the growth in this area of the budget. The amount to restore the position is $88,538 of which $22,135 is general funds.
- The Department requested that the House add additional funds to the outpatient line item due to a calculation error that was made at the time the budget was prepared. The House agreed to increase the budget by $6.3 million of which $2.2 million were general funds.
- The House reduced the drug line item by $2.8 million of which $1.0 million is general funds. While the Department through a series of measures were actually able to reduce drug costs during the 2003 state fiscal year, the cost increased by 12.7% in 2004. The Executive Budget request was an $11.9 million increase over the appropriation for the current biennium, of which about $8.2 million are general funds. This is only an increase of about 6.1% per year. We believe the requested increase is necessary and ask that you consider reinstating this funding to the Medicaid Program budget.
- Another reduction was made to the Home Health Agency service request by $100,000 in general funds, and the optometric request by $50,000 in general funds. Based on the most current trend information that was not available at the time the budget was prepared, these reductions appear reasonable and are acceptable to the Department.
- The House added $565,000 of which $282,500 is general funds to implement the provisions contained in House Bill 1459 regarding a disease management program for the 2,000 highest cost recipients in the Medicaid Program. Also adjusted downward the Medicaid grants by $1.5 million of which about $537,000 is general funds to offset the anticipated savings that will occur as a result of disease management activities. The Department supports this concept.
- A reduction was made in the Community Health Care Trust Fund to the level of the appropriation for the current biennium. This fund provides the non-federal matching dollars for the breast and cervical cancer services provided to women that are eligible for the Women's Way Program. This program provides Medicaid coverage to women with cancer who have no other coverage. The Legislature authorized this service during the 2001 session. We are required to provide all needed services for these women and will need to use general fund dollars if the trust fund dollars are not sufficient to cover the non-federal share of the cost of this program. We request that the consider restoring the funding to the amount requested in the Executive Budget.
- The House added about $171,000 of which $60,000 is general funds to provide fee increases specifically for air and ground ambulance services.
- The House reduced the Medicaid grants line item by $252,000 of which $91,000 are general funds due to reducing the proposed increase in funeral accounts from $5,500 to $5,000. The current limit is $3,000 for each Medicaid recipient. The cost to raise the funeral allowance to $5,500 was included in the Executive budget.
I would be happy to respond to any questions you may have.
Attachments
- A: Medicaid enrolled by age group Attachment (100kb jpg)
- A1: Number of Medicaid enrolled by age group Attachment (76kb jpg)
- B: Comparison of net Medicaid Eligibles and unduplicated recipients Attachment (56kb gif)
- C: Healthy Steps Children's Health Insurance Program enrollment by month Attachment (20kb gif)
- D: Medical Services 2003-2005 and 2005-2007 Budget Biennium Comparisons Attachment (156kb jpg)
- D1: Medical Services 2003-2005 and 2005-2007 Budget Biennium Comparisons continued Attachment (184kb jpg)
- D2: Medical Services 2003-2005 and 2005-2007 Budget Biennium Comparisons continued (128kb jpg)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![]() Top of page
Top of page ![]() Back to previous page
Back to previous page